Overview – Biopsychology
Biopsychology is the study of psychology from the perspective of the underlying biology (i.e. it’s the biological approacha from the approaches topic). But where the approaches section focused mainly on genetics, this biopsychology section drills down more into the physiology and biochemistry underlying behaviour:
- The nervous system (including neurons and the divisions of the nervous system)
- The endocrine system (including glands and hormones such as adrenaline)
- The brain (including the different areas of the brain and ways of studying the brain)
- Biological rhythms
Note: A level students need to understand all these topics. AS students only need to understand the first 2 – i.e. they do not need to learn about the brain’s physiology or biological rhythms.
The nervous system
The nervous system is the main system that controls the mind and body. It takes in information from the environment and elsewhere in the body (transmitted across neurons) and co-ordinates a wide range of conscious functions such as thinking and movement, as well as unconscious functions like the control of organs (e.g. heart rate, digestion) and glands.
Divisions of the Nervous System
In humans (and other vertebrate animals), the nervous system is divided into two parts: the central nervous system (CNS) and peripheral nervous system (PNS). These two parts are divided into further subcategories:
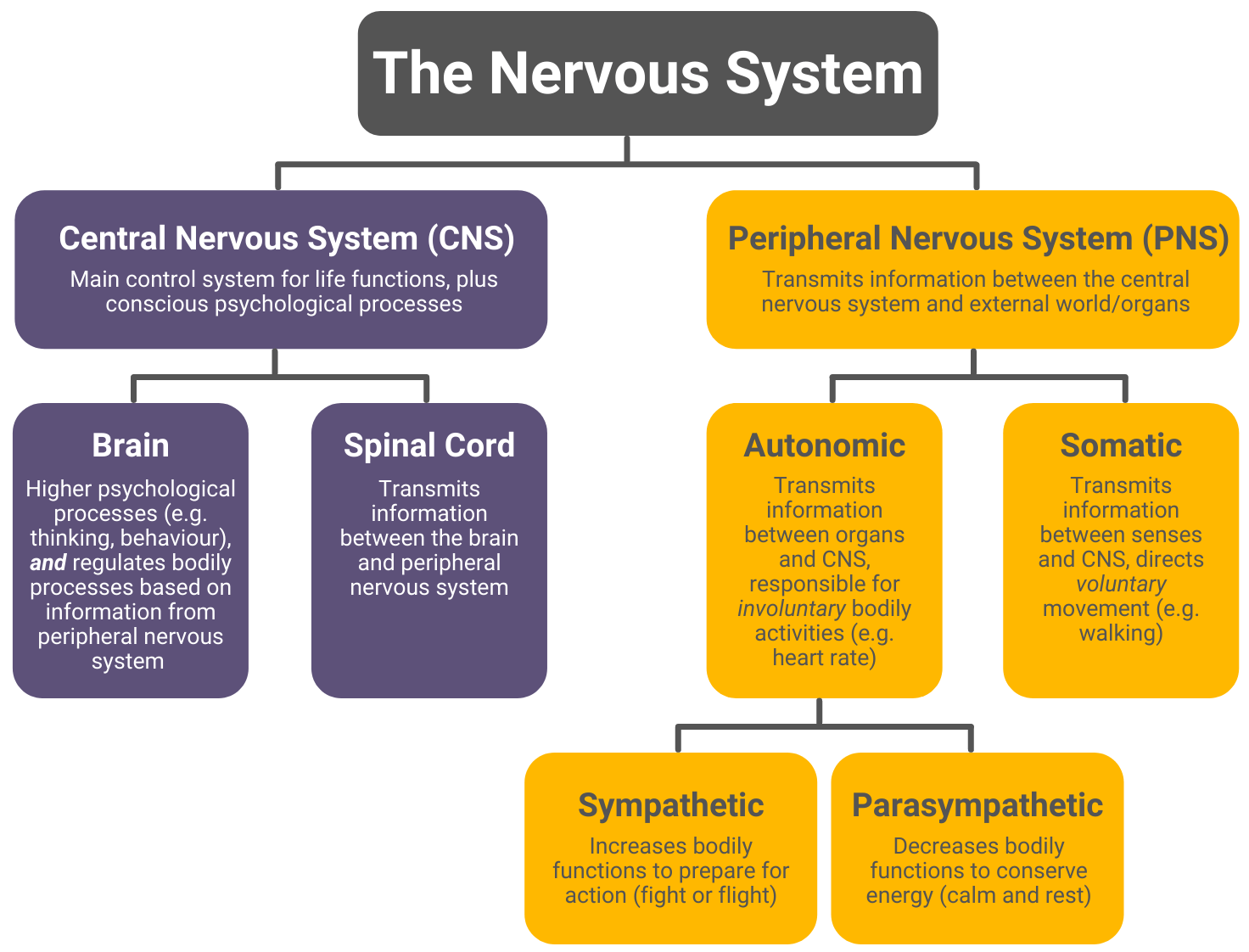
Central Nervous System
The central nervous system is the main control system of the body. It consists of two parts: the brain and spinal cord.
Brain
In addition to obvious functions like thinking, the brain is also responsible for:
- Perception (i.e. translating information from the senses so it can be understood and processed)
- Motor control (i.e. sending commands to muscles to move)
- Regulating bodily processes and maintaining homeostasis (e.g. maintaining temperature and hormone levels based on information from the peripheral nervous system)
- Sleep
Spinal cord
The spinal cord connects the brain with the peripheral nervous system. In other words, it connects the brain with the rest of the body and with the external world. The spinal cord is also responsible for some unconscious movements, such as reflexes (e.g. the one where you get hit on the knee and your leg kicks).
Peripheral Nervous System
The peripheral nervous system goes beyond the central nervous system to connect it with the rest of the body and the external world. It consists of two parts: the somatic nervous system and the autonomic nervous system.
Somatic
The somatic nervous system is responsible for voluntary movement (e.g. walking). It transmits information between the central nervous system and the senses (i.e. it connects the brain to the external world) and is under conscious control.
Autonomic
The autonomic nervous system is responsible for transmitting information between the central nervous system and the internal organs (i.e. it connects the brain to the rest of the body). Unlike the somatic nervous system, it is involuntary and not under conscious control.
The functions of the autonomic nervous system can be divided into two categories: sympathetic and parasympathetic, which oppose each other. For example:
In general, sympathetic functions increase bodily activity to prepare for action – an example of this is the fight or flight response. In contrast, parasympathetic functions decrease bodily activity to conserve energy.
Neurons
Neurons are the main components of the nervous system. They are how information is transmitted from one part of the nervous system to another. There are around 100 billion neurons in the brain and another 1 billion in the spinal cord.
Although there are different types of neurons, they all have the same general structure:
- The dendrite (receptor) receives a signal
- The signal is carried towards a cell body (which contains the nucleus)
- The signal travels along an axon (which is protected by myelin sheaths) towards the axon terminal
- Terminal boutons at the end of the axon pass the electrical signal to the next neuron in the chain
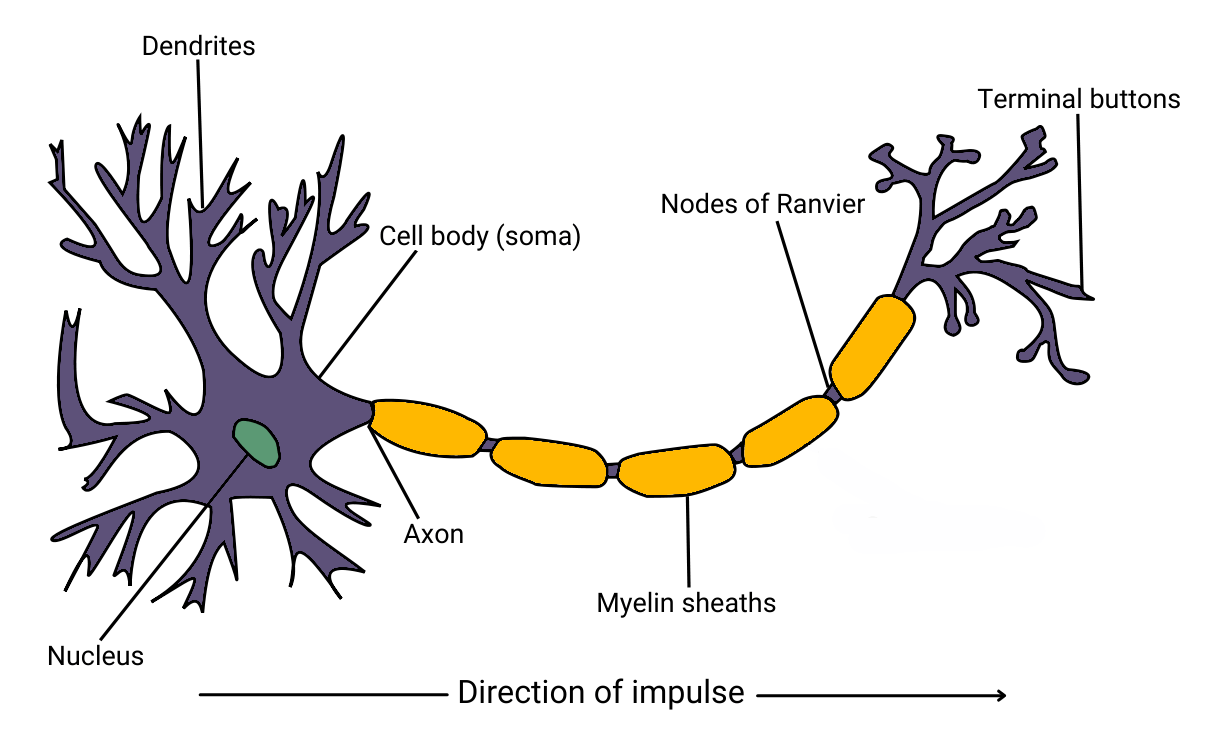
Signals are passed within neurons electrically. At rest, the neuron is negatively charged but becomes positively charged when activated, which sends an electrical impulse through the axon.
Once this electrical signal reaches the axon terminal, synaptic transmission enables the signal to pass along to the next neuron in the chain.
Synaptic Transmission
Neurons are separated by small gaps called synapses, and synaptic transmission is the process of sending information from one neuron to another.
The gap between two neurons is called the synaptic cleft (or synapse). When the electrical signal within a neuron reaches the axon terminal of that neuron, neurotransmitters are released from vesicles and cross over the synapse where they are taken up by receptors in the dendrites of the other neuron.
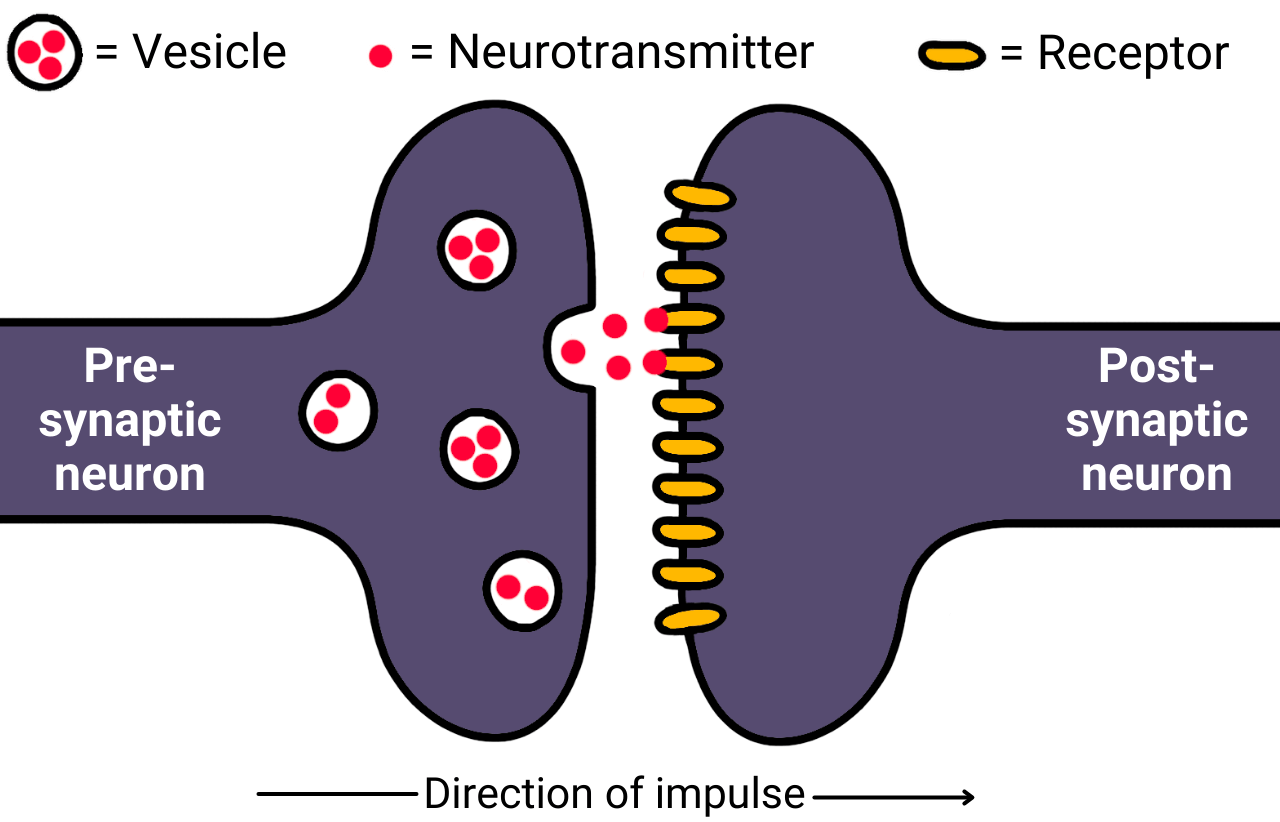
Whereas signals within neurons are transmitted electrically, signals between neurons are transmitted chemically. In other words, neurotransmitters are chemicals. When a neurotransmitter is taken up by the receptor of the next neuron, it is converted back to an electrical signal which passes along the axon of that neuron until it reaches the axon terminal where the chain can continue.
Excitation and inhibition
Neurons contain many different types of neurotransmitters such as serotonin, dopamine, glutamate, GABA, and acetylcholine. These different neurotransmitters can have either excitatory or inhibitory effects:
- Excitatory: Increase the likelihood of the neuron firing
- Inhibitory: Decrease the likelihood of the neuron firing
For example, serotonin has a generally inhibitory effect. When serotonin binds to the receptor of a neuron, it increases the negative charge of that neuron, making it less likely to fire. In contrast, glutamate has an excitatory effect. So, if glutamate outweighs serotonin in a neuron, the net effect is increased likelihood of that neuron firing.
Types of Neurons
Neurons are classified into 3 main types according to their function within the nervous system:
- Sensory neurons: Transmit information from the senses (e.g. the eyes or fingertips) to the central nervous system
- Motor neurons: Transmit information between the central nervous system and the organs and muscles (e.g. an instruction to the adrenals to produce adrenaline)
- Relay neurons: Connect neurons to other neurons (e.g. motor neurons to sensory neurons) and transmit information within the central nervous system (also called interneurons)
The endocrine system
The endocrine system is a system of glands that are responsible for the release of hormones. The pituitary gland (the ‘master gland’) of the endocrine system is linked to the nervous system via the hypothalamus, which co-ordinates and regulates the release of hormones from glands.
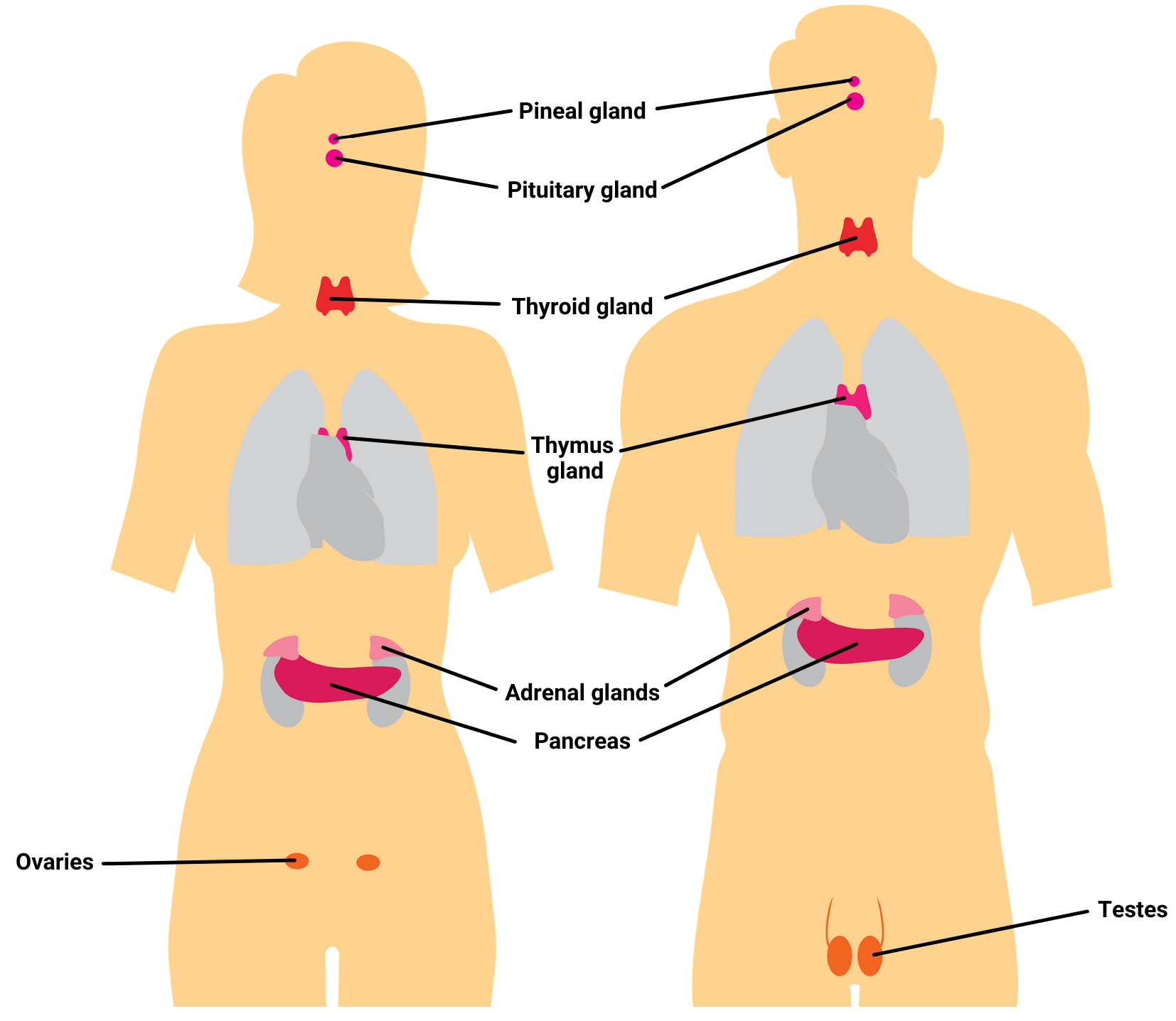
Glands and hormones
Hormones are chemicals that communicate information throughout the body. Different hormones are produced and released by different glands in the body.
The effects of hormones are significant and affect growth, sleep, mood, metabolism, and just about every other process in the body. They flow through the body and bind to specialised receptors in cells (a bit like how neurotransmitters bind to receptors in neurons). When a hormone binds to a receptor, it can cause an effect in that cell. For example:
| Gland | Hormone(s) | Effect(s) |
| Pituitary | Growth hormone Prolactin |
Growth hormone: Stimulates growth and cell division Prolactin: Stimulates milk production (females) |
| Testes | Testosterone | Responsible for male secondary sex characteristics (e.g. body hair, deeper voice, bigger bone structure), sperm cell production, increases aggression and muscle size |
| Ovaries | Estrogen Progesterone |
Estrogen: Responsible for female secondary sex characteristics (e.g. breast development, wider hips), egg maturation Progesterone: Regulates uterus for pregnancy |
| Thyroid | Thyroxine | Increases metabolism, regulates growth and temperature |
| Pineal | Melatonin | Regulates circadian rhythm and sleep |
| Adrenal | Cortisol Adrenaline |
Cortisol: Maintains blood sugar, regulates inflammation and immune response Adrenaline: see below |
The endocrine system transmits information chemically, and operates much more slowly than the nervous system. It is primarily regulated via the pituitary gland (the ‘master’ gland), which connects the endocrine system to the nervous system (via the hypothalamus).
Adrenaline: Fight or Flight
You don’t need to remember all the specific glands and hormones and their effects for A level psychology. Instead, the main one the syllabus focuses on is adrenaline.
Adrenaline is responsible for the fight or flight response: an activation of the sympathetic side of the autonomic nervous system to prepare the body for action. The process for this is as follows:
- The brain (specifically the hypothalamus) senses a threat
- The hypothalamus sends a message to the adrenal glands (specifically the adrenal medulla) to release adrenaline
- Adrenaline increases bodily activities to either fight or flee from the threat
- For example, heart rate increases to improve blood flow, the bronchioles of the lungs dilate to increase oxygen intake, and the pupils dilate to increase vision. Other bodily activities that are not essential for fighting or fleeing are reduced, such as digestion
- Once the brain senses that the threat has passed, the parasympathetic nervous system reduces these activities and returns the body to a resting state (rest and digest rather than fight or flight).
The brain
Note: This topic is A level only, you don’t need to learn about the brain’s physiology if you are taking the AS exam only.
- Areas of the brain, in particular how these different areas are responsible for different functions
- Neuroplasticity and how this enables recovery from brain injury
- Ways of studying the brain
Areas of the brain
Early scientists tended to see the brain in a holistic way, meaning they saw all areas of the brain as used for all functions. More recent (i.e. >20th century) scientists now tend to take a more localised approach. Different areas of the brain appear to be responsible for different functions, and damaging these areas effects those functions.
Hemispheric Lateralisation
 The first way the brain can be divided is laterally, i.e. a left half and a right half. These halves are called hemispheres. Each of the two hemispheres can be further divided into four lobes: frontal, parietal, occipital, and temporal.
The first way the brain can be divided is laterally, i.e. a left half and a right half. These halves are called hemispheres. Each of the two hemispheres can be further divided into four lobes: frontal, parietal, occipital, and temporal.
The two hemispheres are not symmetrical – they do different things. For example, the left hemisphere tends to be more involved in language processing, whereas the right hemisphere tends to be more involved in processing spatial relationships.
As a general rule, information from the left side of the body is processed by the right hemisphere and vice versa (contralateral). For example, damage to the motor cortex in the right hemisphere will affect the person’s ability to move their left side, and damage to the auditory cortex in the left hemisphere will affect a person’s hearing in their right ear.
Split-brain research
The two hemispheres of the brain are connected by a bundle of nerve fibers called the corpus callosum.
In rare cases of extreme epilepsy, a surgeon may cut the corpus callosum (corpus callosotomy), separating the right and left hemispheres from each other. This contains any epileptic seizures to just one side of the brain, reducing their severity.
Despite the dramatic nature of the procedure, patients who’ve undergone a corpus callosotomy (split-brain patients) are able to live relatively normal lives. However, there are some effects on functioning, as observed in Sperry (1968):
- When split-brain patients were shown an image to their right visual field, they were able to describe in words what they saw. However, when they were shown the same image to their left visual field, they were not able to describe what they saw. This is likely because visual information from the left side is processed in the right hemisphere (the visual cortex is contralateral) and language processing primarily occurs in the left hemisphere. So, the visual data in the right hemisphere could not be shared to the language processing areas in the left hemisphere in order for the split-brain patient to describe what they saw.
- However, despite not being able to describe in words the image shown to the left visual field, the split-brain patients could use their hands to pick an object associated with that image. For example, if the split brain patient was shown a cigarette to their left visual field, they could use their left hand to pick an ashtray. This can be explained by the fact that the left hand is controlled by the right hemisphere (again, the motor cortex is contralateral) and the image that was shown to the left visual field would have been processed in the same (right) hemisphere.
AO3 evaluation points: Split-brain research
Strengths of split-brain research:
- Evidence supporting hemispheric lateralisation: Sperry’s experiments demonstrate that brain functions are lateralised. For example, if images processed in the right hemisphere can’t be spoken of, this suggests that the image processing and language processing do indeed happen in different hemispheres.
Weaknesses of split-brain research:
- Methodological concerns: Split-brain patients are rare (just 11 participants took part in Sperry’s experiments) and as such we should be cautious about applying findings from them to the entire population. This issue is further compounded by the fact that split-brain patients are already anomalous prior to the corpus callosotomy procedure: They undergo this procedure because they suffer from epileptic fits. How do we know, for example, that the effects seen in Sperry’s experiments are effects of splitting the hemispheres rather than effects of epilepsy itself, or drugs used to treat epilepsy? These methodological concerns raise questions about the validity of the conclusions drawn.
- Conflicting evidence: Some case studies conflict Sperry’s findings. For example, Gazzaniga (1998) describes how a split-brain patient, J.W., learned to speak about information presented to his right hemisphere 13 years after undergoing a corpus callosotomy. Similarly, Danelli et al (2013) – see functional recovery after trauma below – describes the case study of a boy who had his entire left hemisphere removed and yet learned to speak. These examples weaken the case for hemispheric lateralisation because they show how functions associated with a single hemisphere (language is associated with the left hemisphere) can actually be performed by both hemispheres.
- Overly simplified: Sperry’s research often leads to the exaggeration and oversimplification of the different functions of the left and right hemispheres. In reality, functions associated with one hemisphere (e.g. the left) can be carried out or shared by the other hemisphere when necessary.
Localisation of brain function
Localisation of function refers to identifying specific areas of the brain that correspond to specific functions. For example, damage to the auditory cortex in the brain can damage hearing, whereas damage to the motor cortex may reduce a person’s ability to move. This suggests these functions are localised within these areas of the brain.
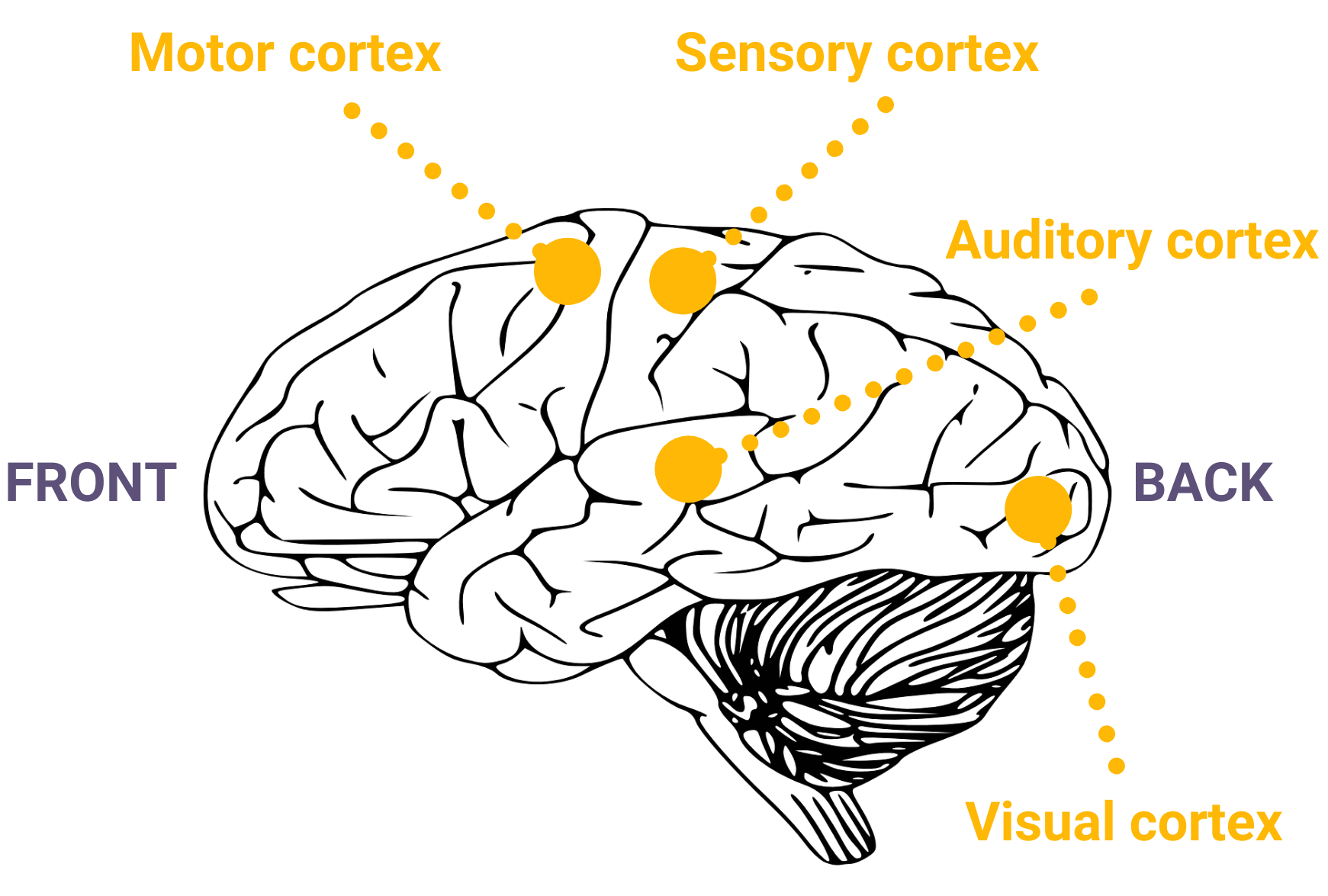
Motor cortex (voluntary movement)
The motor cortex of the brain is responsible for voluntary movement, such as walking. It is located in the frontal lobes of each hemisphere. However, basic involuntary movements (like coughing) are controlled by other parts of the brain.
So, damage to the motor cortex may limit a person’s motor skills. For example, a person with a damaged motor cortex may have difficulty holding a pen.
Somatosensory cortex (touch)
 The somatosensory cortex of the brain is responsible for sensing physical sensations on the skin, like pressure and heat. It is located in the parietal lobes of each hemisphere.
The somatosensory cortex of the brain is responsible for sensing physical sensations on the skin, like pressure and heat. It is located in the parietal lobes of each hemisphere.
The number of neurons in the somatosensory cortex differs according to body part. For example, there are many more neuronal connections dedicated to processing information from the hands than the ankles because people use their hands to feel things much more commonly than they do their ankles.
Visual cortex (seeing)
 The visual cortex of the brain is responsible for processing visual information from the eyes. It is located in the occipital lobes of each hemisphere. The visual cortex is contralateral: The right hemisphere processes data from the left of a person’s field of vision (both eyes) and vice versa.
The visual cortex of the brain is responsible for processing visual information from the eyes. It is located in the occipital lobes of each hemisphere. The visual cortex is contralateral: The right hemisphere processes data from the left of a person’s field of vision (both eyes) and vice versa.
So, damage to the visual cortex of the right hemisphere may make it difficult for a person to perceive objects to the left of them.
Auditory cortex (hearing)
 The auditory cortex of the brain is responsible for processing sound. It is located in the temporal lobes of each hemisphere. The auditory cortex is also contralateral: The right hemisphere processes sound from a person’s left ear and vice versa.
The auditory cortex of the brain is responsible for processing sound. It is located in the temporal lobes of each hemisphere. The auditory cortex is also contralateral: The right hemisphere processes sound from a person’s left ear and vice versa.
So, damage to the auditory cortex of the left hemisphere may cause hearing difficulties in a person’s right ear.
Language centres
As mentioned, language processing primarily happens in the left hemisphere. There are two areas that are particularly important for language: Broca’s area and Wernicke’s area.
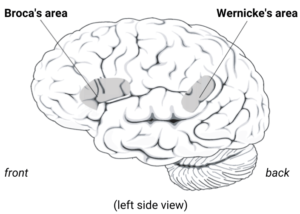
Broca’s area (speech production)
The Broca’s area is the main area where speech is produced. It is located in the frontal lobe of the left hemisphere.
The Broca’s area was identified by and named after Pierre Paul Broca in the mid 19th Century. From post-mortem autopsies, Broca observed that patients who’d had difficulty producing words had lesions (damage) in this area of the brain.
Damage to the Broca’s area causes Broca’s aphasia (also called expressive aphasia), a condition characterised by slow speech, lack of fluency, and an inability to find the right words. Despite difficulties producing speech, people with Broca’s aphasia often have normal language comprehension – i.e. they understand what others are saying.
Wernicke’s area (speech comprehension)
Another important (but separate) area for language is Wernicke’s area. The Wernicke’s area is primarily responsible for language comprehension (both written and spoken). It is located in the temporal lobe.
Damage to the Wernicke’s area causes Wernicke’s aphasia (also called receptive aphasia). Patients with Wernicke’s aphasia typically have no problems producing speech – they speak in a fluent and effortless way – but the content of what they say often lacks meaning.
AO3 evaluation points: Localisation of function
Strengths of localisation of function:
- Evidence supporting localisation of function:
- Case studies: Several case studies support the claim that different functions within the brain are localised in specific areas. Perhaps the most famous example is Phineas Gage, a 19th century railroad worker. Gage had an iron bar shot straight through his head during an accident while working, which damaged the left frontal lobe of his brain. Before the accident, Gage was calm and polite, but after the accident Gage was violent and rude (however, some accounts claim these characterisations are exaggerated). Gage’s doctor believed the damaged area (the left frontal lobe) was responsible for self-control, which was confirmed by later research into localisation of function.
- Brain scans: fMRI scans demonstrate correlations between different mental activities and different areas of the brain. For example, Ovaysikia et al (2011) demonstrates increased blood flow in different areas of the brain depending on whether a person is reading words or recognising facial expressions.
Weaknesses of localisation of function:
- Higher cognitive processes: Higher cognitive processes such as learning, language, and memory are seemingly too complex to be localised within a single area. For example, Lashley (1950) removed different parts of rats brains while they were learning a maze but found no single area was most important. This suggests higher cognitive processes (e.g. learning) are distributed in a holistic way within the brain, rather than being localised in a single area.
- Neuroplasticity: The fact that the brain can recover functions after damage to areas associated with that function suggests that mental activities are not localised in these areas. For example, language is supposedly localised within the the left hemisphere, but Danelli et al (2013) – see functional recovery after trauma below – describes the case study of a boy who had his entire left hemisphere removed and yet learned to speak.
- Methodological concerns: Cases studies (e.g. Phineas Gage) use a sample size of just one and so it may not be valid to generalise findings from case studies to the entire population of human beings.
Neuroplasticity
Just like how plastic can be moulded and shaped, so too can the brain: New neuronal connections can be formed and old ones removed. Neuroplasticity is this ability of the brain to change its physical structure to perform different functions.
In childhood, the brain is highly plastic. This plasticity enables infants and children to quickly learn new skills, adapt to their environment, and recover from brain injury. Neuroplasticity reduces with age, but still remains: Unused pathways are removed, commonly used pathways are strengthened, and new pathways can be formed.
Functional recovery after trauma
Neuroplasticity enables people to recover function after trauma (e.g. brain damage caused by stroke or accident). To recover function, the brain restructures itself in the following ways:
- Other areas of the brain adapt to take over the function of damaged areas: For example, Danelli et al (2013) describes a case study of a boy who had his entire left hemisphere removed at age 2 and a half. As described above, language function is primarily localised in this hemisphere, and the boy was initially unable to speak. However, his language skills recovered after 2 years, suggesting the right hemisphere adapted to take over this function.
- Unused neural pathways are recruited: Wall (1977) observed that the brain contains many dormant neural connections. When healthy neural connections are damaged, these previously dormant synapses activate and form new connections to compensate for the damaged ones.
- Axon sprouting: Damage to the axon of a neuron can break its connections to neighbouring neurons. When this happens, the neighbouring intact neurons may grow (‘sprout’) extra nerve endings to reconnect with these damaged neurons.
AO3 evaluation points: Neuroplasticity
- Evidence supporting neuroplasticity: Several studies demonstrate the brain’s ability to change its physical structure to perform different functions. In addition to the studies above, brain scans by Maguire et al (2000) found that London taxi drivers had a higher volume of grey matter in the posterior hippocampus (an area associated with spatial memory and navigation) compared to controls. This suggests this area of the brain adapted in cab drivers to help them with their work.
- Variations between people: Neuroplasticity and the ability of the brain to recover function after damage differs depending on several factors, such as:
- Age: The brain tends to lose neuroplasticity with age. For example, Danelli et al (2013) demonstrates that young people can recover function even after extensive damage to the brain, but it’s highly unlikely that an older patient could recover from such extensive damage. However, Bezzola et al (2012) found evidence of neural changes in participants aged 40-60 following 40 hours of golf training. This suggests neuroplasticity still exists to some extent even among older adults.
- Gender: Some research (e.g. Ratcliff et al (2007)) suggests women are better able to recover function after brain damage than men. A possible explanation of this is that female brains have (on average) more neural connections between the left and right hemispheres than men, resulting in more distributed use of both hemispheres. This reduced hemispheric lateralisation would mean the other hemisphere is better able to compensate for the functions of the damaged hemisphere.
Ways of Studying the Brain
There are many ways psychologists and scientists study the brain. These methods are used to better understand how the brain works (e.g. where functions are localised) and diagnose and treat illness.
fMRI
Functional magnetic resonance imaging (fMRI) is a form of brain scanning. It uses magnetic fields to measure blood flow and oxygenation in the brain.
When an area of the brain is highly active, that area needs more oxygen and greater blood flow to provide this oxygen. By measuring blood flow and oxygenation, fMRI scanners enable researchers to identify which areas of the brain are activated during certain tasks.
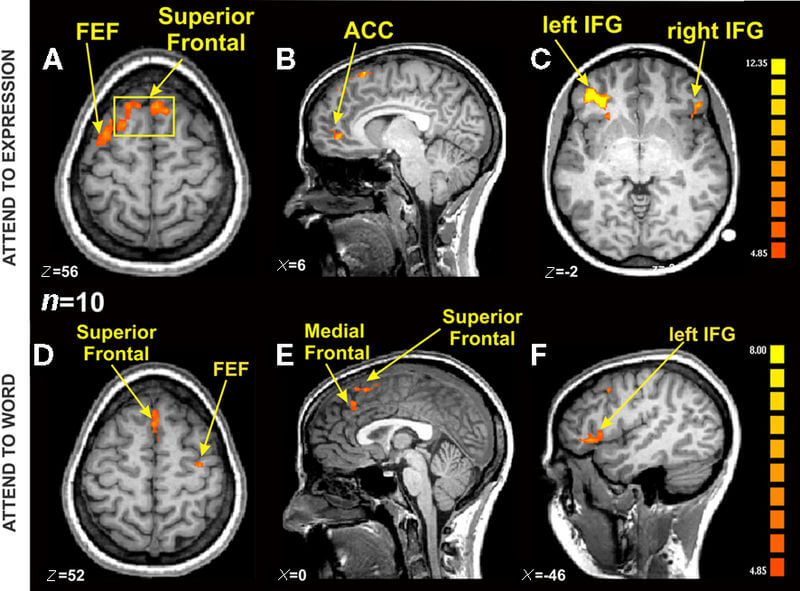
The example fMRI scans above are from Ovaysikia et al (2011). In this study, the researchers measured brain activity during two tasks: Reading words and recognising facial expressions. As can be seen from the fMRI scan above, the different tasks increased brain activity in different areas.
AO3 evaluation points: fMRI
Strengths of fMRI:
- Dynamic: fMRI scans record brain activity as it happens, which enables researchers to see activity in the brain over time (unlike post-mortem). For example, when a person switches from working out a maths equation to thinking about a childhood memory, fMRI scanners can pick up the change in brain activity.
- High spatial resolution: fMRI scans are able to identify activity in the brain to within 1mm. This provides a highly detailed and accurate picture of brain activity (much more so than EEG).
Weaknesses of fMRI:
- Expensive: fMRI scanners are expensive to buy and maintain (compared to EEG). This limits their use as psychological research tools, with studies that do use fMRI scanners often consisting of small sample sizes in order to reduce costs.
- Low temporal resolution: It takes several seconds between recording brain activity using fMRI and converting it into an image. This means fMRI generates fewer images per minute (compared to e.g. EEG) and brain activity between each image is not recorded.
Electroencephalogram and ERPs
 An electroencephalogram (EEG) is a scan of the brain’s electrical activity. An EEG scan is performed by attaching electrodes to the scalp or by using a hat with electrodes attached.
An electroencephalogram (EEG) is a scan of the brain’s electrical activity. An EEG scan is performed by attaching electrodes to the scalp or by using a hat with electrodes attached.
The electrodes detect electrical activity in the brain cells beneath them. So, the more electrodes that are used in an EEG, the more complete a picture of brain activity the EEG can provide.
Event-related potentials (ERPs) are closely related to EEG scans. They use the same equipment but use statistical techniques to measure changes in brain activity in response to a stimulus. For example, the EEG could initially provide a baseline picture of brain activity, then researchers could introduce a stimulus (e.g. giving a subject some food to eat) and use ERPs to determine how brain activity changed in response.
AO3 evaluation points: Electroencephalogram and ERPs
Strengths of EEG and ERPs:
- Dynamic: Like fMRI, EEG and ERPs enable researchers to measure changes in brain activity as they happen.
- Lower cost: EEG brain scans are much less expensive than fMRI brain scans.
- Higher temporal resolution: EEG can record several pictures of the brain per second, unlike fMRI.
Weaknesses of EEG and ERPs:
- Low spatial resolution: The electrodes of EEG only measure general electrical activity and are unable to provide a detailed view of what is happening in the brain (unlike fMRI). For example, neurons associated with feeling in the hands may be next to neurons associated with hearing, but the EEG will not be able to differentiate between the two. However, some psychological conditions have distinctive electrical signals (e.g. epilepsy) and so EEGs are useful diagnostic tools for them.
Post-mortem
 A post-mortem is a physical examination of the brain after a person has died. By physically analysing a brain (for example, by weighing it, dissecting parts of it, and comparing it to neurotypical (‘normal’) brains) and cross-referencing this with the person’s behaviour in life (e.g. any psychological disorders the person had) the examiner can learn more about the causes of behaviours and psychological disorders.
A post-mortem is a physical examination of the brain after a person has died. By physically analysing a brain (for example, by weighing it, dissecting parts of it, and comparing it to neurotypical (‘normal’) brains) and cross-referencing this with the person’s behaviour in life (e.g. any psychological disorders the person had) the examiner can learn more about the causes of behaviours and psychological disorders.
An example of this is described above: From post-mortem analysis of the brains of patients with speaking difficulties, Pierre Paul Broca identified that the Broca’s area of the brain is important for speech production.
AO3 evaluation points: Post-mortem
Strengths of post-mortem:
- Post-mortems enable researchers to study deeper areas of the brain that cannot be reached, for example, by EEG.
Weaknesses of post-mortem:
- No brain activity: As the person is dead, a post-mortem does not enable researchers to measure dynamic brain activity (unlike fMRI and EEG). As such, researchers may have to speculate about (rather than measure) connections between the person’s physical brain and their psychological character (e.g. psychological conditions) when they were alive.
Biological rhythms
Note: This topic is A level only, you don’t need to learn about biological rhythms if you are taking the AS exam only.
The activities of the mind and body follow various cycles, which are known as biological rhythms. These biological rhythms are categorised in the following ways:
| Category | Length | Example |
| Circadian | 24 hours | Sleep and wake cycle |
| Infradian | More than 24 hours | Female menstrual cycle |
| Ultradian | Less than 24 hours | Stages of sleep |
Biological rhythms are controlled by endogenous pacemakers, which are influenced by exogenous zeitgebers:
- Endogenous pacemakers: Things within the body that regulate biological rhythms (your ‘body clock’).
- E.g. The suprachiasmatic nucleus of the hypothalamus
- Exogenous zeitgebers: Cues in the external environment that inform endogenous pacemakers to regulate biological rhythms.
- E.g. Sunlight and darkness prompt the body to release hormones that control sleep and wake cycles
AO3 evaluation points: Endogenous pacemakers and exogenous zeitgebers
- Examples of the effect of exogenous zeitgebers: Campbell and Murphy (1998) conducted an experiment where participants were woken up in the middle of the night. After waking, one group had light shone onto the back of their knees whereas the control group went through the same procedure but the lightbulb was unplugged. The researchers observed that the group who’d had light shone on the backs of their knees had a greater deviation from their original circadian rhythm compared to the control group. This demonstrates the importance of the exogenous zeitgeber of light (even when shone on the skin rather than the eyes) for regulating circadian rhythm.
- Examples of the effect of endogenous pacemakers: Ralph et al (1990) transplanted cells from the suprachiasmatic nucleus of hamsters with a 20-hour circadian rhythm into normal hamsters with a 24-hour circadian rhythm. This shortened the circadian rhythms of these hamsters to 20 hours from 24, which illustrates the importance of this endogenous pacemaker in maintaining circadian rhythms. However, as an animal study, these findings may not be valid when applied to humans.
- Relative importance: Endogenous pacemakers appear to be more important than exogenous zeitgebers in regulating circadian rhythms. There are many studies where circadian rhythms remain regular despite significant disturbances to exogenous zeitgebers (see the AO3 evaluation points for circadian rhythms for examples).
Circadian
Circadian rhythms are biological cycles lasting approximately 24 hours. An example of a circadian rhythm is the sleep/wake cycle: You might cycle between sleeping for 8 hours when it gets dark and being awake for 16 hours during the day, for instance.
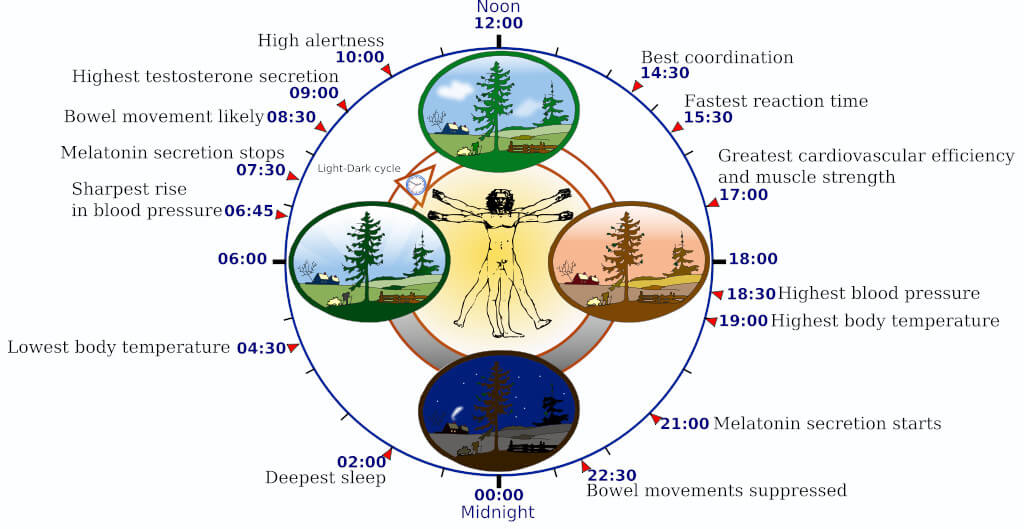
Examples of endogenous pacemakers that control circadian rhythm include systems that release hormones such as melatonin, systems that regulate body temperature, and systems that control metabolism and digestion. The main system that controls circadian rhythms is the suprachiasmatic nucleus (SCN).
These internal processes are influenced by exogenous zeitgebers – perhaps the most obvious of which is sunlight. For example, the darkness of night is thought to trigger melatonin release, which makes you feel tired and want to go to bed.
AO3 evaluation points: Circadian rhythms
- Endogenous pacemakers appear to be more important than exogenous zeitgebers in regulating circadian rhythms. There are many studies where circadian rhythms remain regular despite significant disturbances to exogenous zeitgebers. For example:
- Speleologist Michael Siffre conducted several case studies (using himself as a subject) on the effects of living in a cave without the exogenous zeitgeber of natural light. In 1962, he spent two months in a cave without any natural light and without a clock. Then, in 1975, he conducted a similar experiment but for six months. In both experiments, Siffre maintained a regular sleep/wake cycle and circadian rhythm of around 25 hours.
- Aschoff and Wever (1976) conducted an experiment where participants were kept in a World War 2 bunker without any natural light for four weeks. All participants (except one) maintained a circadian rhythm very close to 24 hours, despite the absence of natural light.
- Folkard et al (1985) conducted a similar experiment where participants were kept in a cave without sunlight for three weeks. The participants were supposed to go to bed when a clock said 11:45pm and wake when it said 7:45am, but unbeknown to them the researchers slowly increased the clock speed so that what seemed like a 24-hour day was actually only 22 hours. Despite these faster clocks, all but one participant maintained a consistent 24 hour circadian rhythm.
- Practical applications: Understanding circadian rhythms can help improve the sleep and health of shift workers, for example. Czeisler et al (1982) found that employees whose shifts were stable over 21 days or more had greater employee satisfaction, improved health estimates, and were less likely to leave their job than employees whose work schedules changed every week. This is likely because keeping shift schedules over 21 days or more allowed workers’ circadian rhythms to adjust to their work schedules. This knowledge can be used by businesses that employ workers on shifts to improve employee satisfaction and reduce employee turnover.
- Methodological concerns: Much of the research on circadian rhythms is in the form of case studies or experiments using small sample sizes. As such, these findings may not be valid when applied to the general population.
Infradian
Infradian rhythms are biological cycles lasting more than 24 hours. An example of an infradian rhythm is the human menstrual cycle: Women typically ovulate once every 28 days.
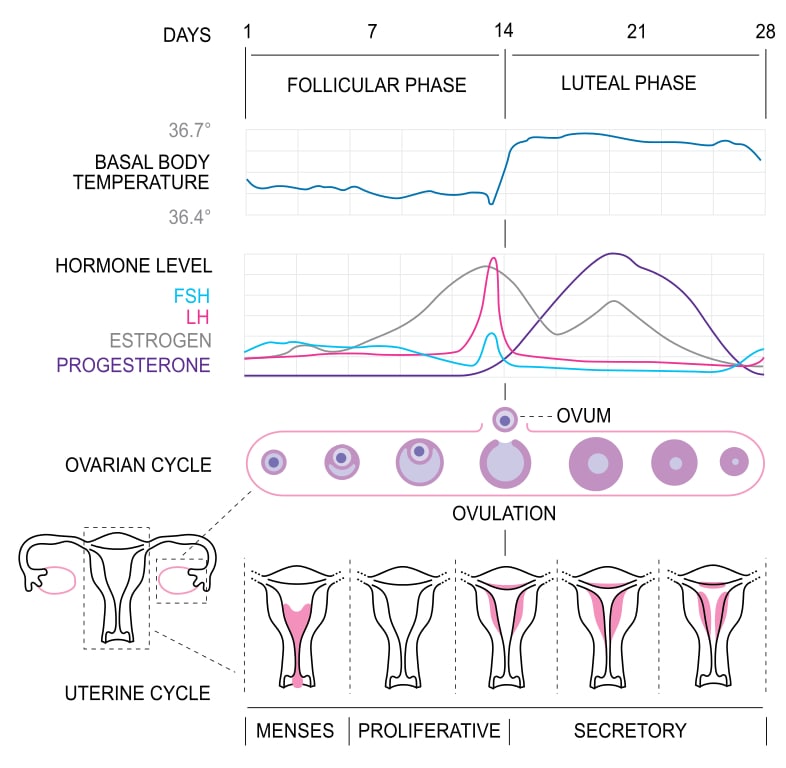
As with circadian rhythms, infradian rhythms are controlled by endogenous pacemakers. For example, hormones such as estrogen and progesterone are crucial to the menstrual cycle.
Infradian rhythms can also be influenced by exogenous zeitgebers. For example, Stern and McClintock (1998) demonstrated that women’s menstrual cycles change when exposed to pheromones from other women.
Ultradian
Ultradian rhythms are biological cycles lasting less than 24 hours. An example of an ultradian rhythm is the different stages of sleep: During the night, a sleeping person will typically cycle between five stages:
| Stage | Length | Description |
| 1 | 5-15 minutes | Light sleep. Alpha waves increase and brain activity starts to reduce. Heart rate slows and muscles relax. |
| 2 | 5-15 minutes | Light sleep. Brain activity reduces but with occasional bursts of activity. |
| 3 | 5-15 minutes | Deep sleep. Delta brain waves increase and brain activity is greatly reduced. |
| 4 | ~40 minutes | Deep sleep. Delta waves peak, lowest level of brain activity during the sleep cycle. |
| Rapid eye movement (REM) | >15 minutes | High level of brain activity. Dreams are likely to occur. Body is completely relaxed. |
One complete sleep cycle through all these stages will typically take around 90 minutes. So, during a full night’s sleep, a person may repeat this cycle four or five times.